Dr. Joseph Mele, MD, FACS, is a Board Certified Plastic Surgeon, who specializes in Cosmetic Plastic Surgery of the breasts. A significant portion of his San Francisco Bay Area Plastic Surgery practice is dedicated to Breast Augmentation Revision. As many as 25% of all Breast Augmentation patients will have Breast Augmentation Revision within 10 years of their original surgery. The most common reason that a Breast Augmentation is revised is to change size. Other common reasons include: breast implant deflation, capsular contracture, breast implant malposition and rippling. Breast implant infection and exposure can also occur; however, this is more common for breast reconstruction than for Cosmetic Breast Augmentation.
Breast Augmentation Revision Before and After Photos





.jpg)



.jpg)







.jpg)




.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)

.jpg)
.jpg)
.jpg)
.jpg)
Breast Augmentation Revision – Frequently Asked Questions
Breast Implant Revision covers a wide variety of procedures. From simple Breast Scar revisions to complex Breast Augmentation/Lift redos and complete Breast Reconstruction. Approximately 25% of all women who have Breast Augmentation will also have a Breast Augmentation Revision within 10 years of their original surgery. Some are elective, like changes sizes, and some are necessary, like replacing a deflated Breast Implant.
The Breast Augmentation Revision Pages on the San Francisco Breast site are organized by topic, and centered around the most frequently asked questions heard in my San Francisco Bay Area Breast Enhancement private practice. The questions that follow link to the related topic section on this page. With in these sections are links to expanded information available on pages dedicated to each aspect of Breast Augmentation Revision. Additional links to related topics are available at the top of this and each of the Breast Augmentation Revision Pages.
Breast Augmentation Revision Videos
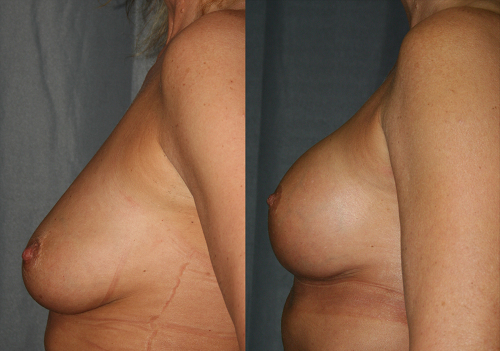
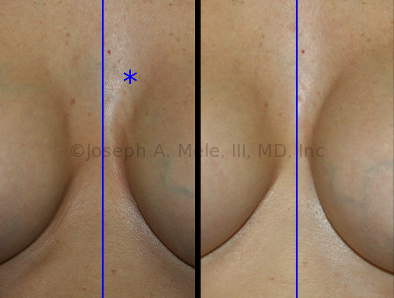
The most common reason for Breast Augmentation Revision is to change Breast Implants. A large number of Breast Implant Exchanges are elective, although Breast Implant Replacement after Breast Implant Deflation (see next section) also occurs. Breast Implant Replacement, when there is nothing wrong with your current Breast Implants, is completely elective. By definition, Elective Breast Implant Replacement is not being performed to fix a problem with the current Breast Implants. The most common reason for Elective Breast Implant Replacement is to change size. The vast majority of these changes are to increase size, but there are times when decreasing the size is also desirable. Small changes in volume to Saline Filled Breast Implants may be possible, without changing the implants themselves. In some cases, additional saline can be added to or removed from the lumen of the Breast Implant. The results are not dramatic, and the adjustment still requires surgery, as implant sterility needs to be maintained. Elective Breast Implant Replacement Before and After Pictures Left: Before breast augmentation. Middle: After breast augmentation with 420cc breast implants. Right: After breast implant replacement with 565cc implants. Breast Implant Replacement when there is a problem with the Breast Augmentation due to limitation of current Breast Implants. In the case of Semi-Elective Breast Implant Replacement, the Breast Implant has not failed, but there is some aspect to the Breast Augmentation result that we want to improve. The semi-elective procedures do not have any medical indications, so they are still elective surgery. Semi-Elective Breast Implant Replacement Before and After Pictures Left: Before breast implant replacement, the implants are low profile, small and uneven due to mild capsular contracture. Right: After breast implant replacement and capsule modifications the breasts are perkier, fuller and more symmetrical. The most common type of Semi-Elective Breast Implant Replacement is to change Breast Implants types or styles. Sometimes Saline Breast Implants are palpable (can be felt too easily) or will cause visible rippling. This is common when there is a small amount of natural breast tissue. Small amounts of breast tissue often cannot adequately disguise a Breast Implant, especially a large Breast Implant. Placing the implants behind the muscle can help. As can changing from Saline to Silicone Breast Implants. Silicone filled Breast Implants tend to feel softer, and have a lower incidence of rippling. Newer Silicone Breast Implants have fewer problems with capsular contracture and leakage, compared to their predecessors, as a result, they have become the most popular choice for Breast Augmentation. New Breast Implant profiles have also evolved over the past 10 years. Too much side boob can often be reduced by choosing a narrower implant. Large gaps between breasts may be improved by choosing a wider implant. And for very flat or Breast Reconstruction patients, new teardrop shaped implants can preferentially enhance lower pole fullness. Urgent (Non-Elective) Breast Implant Replacement has specific medical indications. These procedures are best done sooner than later, to reduce the risk of further problems. Most patients do not desire to wait, but some, like deflation of a saline Breast Implant, can be delayed. However, saline Breast Implant replacement is much easier to perform soon after the deflation, before the Breast Implant Capsule begins to close. Urgent Breast Implant Replacement Before and After Pictures Left: Before breast implant replacement, the implants are high, hard, ruptured and surrounded by a long untreated hematoma. The bump at the bottom of the breast is where the hematoma is about to drain through the skin. Right: After capsulectomies, drainage of the hematoma, closure of the lower pocket, capsule modifications and breast implant replacement with a larger cohesive (form-stable) silicone gel breast implant, the breast’s normal shape and feel is restored. Silicone Breast Implant deflation, on the other hand, should not be delayed. Removal of the broken silicone gel filled implant early, helps prevent gel migration and the formation of silicone granulomas (lumps in the breast). This is especially important when a lump is already present. Breast Implant Deflation is discussed in more detail below. More information about Breast Implant Replacement is available on the Breast Implant Replacement Page. Another common reason for Breast Augmentation Revision is Breast Implant Deflation. Like everything else on the planet, Breast Implants can break or wear out. When a Breast Implant requires replacement (as detailed above), it is a good time to consider if there is anything else you would like to improve about your Breast Augmentation. Is the size optimal? Are they placed correctly on the chest? Are they too close? Are they too far apart? Is the shape right? If so, replacing the Deflated Breast Implant with an identical Breast Implant will take care of the problem. If not, a different style or type of implant may give you a better result, and both Breast Implants may be changed. Left: Saline filled breast implants with complete deflation on the left breast implant. Right: Both breast implants were removed and replaced with silicone breast implants. It is easier to tell if you have a deflated Saline Breast Implant than a deflated Silicone Breast Implant. Saline Breast Implants go completely flat, while Silicone Gel Breast Implants may retain their size and shape. For details on the presentation of Breast Implant Deflation and the available treatment options, please visit our Breast Implant Deflation Page. The three FDA approved Breast Implant manufacturers in the US stand behind their Breast Implants with a generous warranties. Each Breast Implant Manufacturer offers lifetime replacement in case your Breast Implant develops a leak. Moreover, financial assistance is available if your Breast Implant leaks within the first ten years after your Breast Augmentation. To compare Breast Implant warranties visit the San Francisco Breast Breast Implant Warranties Page. If you have Breast Implants, and you know your manufacturer, click on the corresponding logo below for Breast Implant Warranty information. Every effort is made to keep the breast implant warranties listed on this site up-to-date; however, manufacturers may change them without notice. Be certain to check your manufacturer’s website for the latest information Breast Implant Capsular Contracture is another common reason for Breast Implant Revision Surgery. The body forms a thin pocket around the Breast Implant, which holds the Breast Implant in place. This pocket is called the Breast Implant Capsule. Without the capsule, the implant would quickly drop below the breast, or move toward the axilla (armpit). Attempts to minimize the formation of Capsular Contracture with intraluminal steroids, demonstrated the importance of the Breast Implant Capsule. The steroid was too effective, and the practice caused some of worst bottoming-out ever seen. Putting steroids inside the Breast Implant is not a good idea; moreover, the use of intraluminal steroids are not approved by the FDA, because Breast Implants are not drug delivery devices. Usually the capsule is soft, and cannot be felt; however, when the capsule becomes thick or tight, it can cause problems. If the capsule contracts it can change the shape of the augmented breast, or move the Breast Implant, cause Breast Implant Malposition. The result is termed Capsular Contracture. Breast Implant Capsular Contracture Treatment Before and After Pictures Left: The right breast has Grade III capsular contracture. The implant is squeezed upward as the scar tightens. Right: Capsulotomy and capsulectomy can soften the breast and restore a more symmetrical appearance. The right areola shape and scar were also revised. Capsular Contracture is graded by its clinical presentation. Treatment for Capsular Contracture depends on what problem(s) it is causing. For more details on Capsular Contracture grading and Capsular Contracture treatments, visit San Francisco Breast’s Breast Implant Revision for Capsular Contracture Page. Breast Implant Malposition, as the name implies, means the Breast Implants are in the wrong place. The most common malposition is too high and too far lateral (towards the side). Breast Implants can be too high due to the a relatively small amount of skin below the nipple, or a tight pectoralis major muscle. The they may be high from Capsular Contracture. Lateral malposition is often caused by the shape of the rib cage, but may be due to Breast Implants that are too wide for the chest. Breast Implant Malposition in which the Breast Implants are too close together or too low are less common, but well known by their nicknames. Inferior malposition, the Breast Implant sitting too low on the chest, is called “Bottoming-Out“, and also may cause a “Double-Bubble“. While Implants too close together can cause “Symmastia“, “Bread-Loafing“ or a “Mono-Boob“, as what should be two separate breast mounds begin to merge into one. Breast Augmentation Revision Surgery for Malposition Before and After Pictures Left: The right breast is too high and too medial (close to the middle). The most common cause for this is capsular contracture. Right: The right breast implant has been repositioned lower and more lateral with improved symmetry. More information about Breast Implant Malposition is available on the Breast Implant Revision Surgery page dedicated to Breast Implant Malposition. Wrinkling of the outer shell of a Breast Implant is normal. A soft shell, around a soft center, will bend. This is beneficial, because it takes a soft Breast Implant to enlarge the breast, without making a harder breast. Softer Breast Implants are more difficult to feel, and give a more natural result. On the other hand, a hard solid Breast Implant can’t fold, but feels like a rock. When the folds in the implant become visible, this is called rippling. Breast Implant Rippling is almost always present to a small extent. The rippling itself is not harmful, and is not associated with higher rates of Breast Implant Deflation. Mild forms of rippling, most commonly seen on the sides of the breasts, may not be worth treating. When rippling occurs in less subtle way, or is present on a more exposed surface of the breast, like the upper or inner breast, Breast Implant Revision Surgery may be helpful. More information on Breast Implant Revision Surgery for Rippling is available on the San Francisco Breast Breast Implant Rippling Page. Breast Implant Infection is rare, but it is also one of the few Breast Augmentation emergencies. Breast Augmentation is considered a clean case, and infections occur in 1-2% of all clean cases. Most infections are superficial and clear quickly with oral antibiotics. Deep infections, near the Breast Implant, are less common, but more dangerous. Early treatment can usually prevent a superficial infection from becoming a deep infection, and from spreading to inside the Breast Implant capsule. Once an infection is inside the capsule, the Breast Implant may need to be removed to get the infection to clear. Deep infections are less likely for Cosmetic Breast Augmentation than for Breast Reconstruction, and are less likely for Breast Implants placed behind the muscle (submuscular) than for Breast Implants placed in front of the muscle (subglandular). Breast Implant Infections can be disastrous. This is why, if you have a cold or infection, all elective surgery should be postponed until you are well. It is not worth taking a risk with your health or your Breast Implants. For more information about preventing, identifying and treating Breast Implant Infection, visit our Breast Implant Infection Page. Breast Implant Removal may be desired, or may be required, as described above for a Breast Implant infection, or as a part of Breast Implant replacement. Sometimes a woman wants her Breast Implant removed. Patients have requested Breast Implant Removal after weight gain, to reduce the size of their breasts; prior to pregnancy, to reduce the stretch on the breast skin; and sometimes they were tired of having larger breasts. It is not one of the more frequently performed Breast Implant Revision Surgeries, but it an option that has made some patients very happy. Breast Implant Removal Before and After Pictures Left: The before picture shows a perky breast with good skin tone and no sagging. Right: After the breast implant has been removed, this breast returns to its the orginal size. In this case no breast lift was needed, as she had excellent skin elasticity. The biggest problem with Breast Implant Removal is the loss of support for the breast skin. Just like after pregnancy, when the lactating breasts involutes, the breast shrinks and sags. For smaller implants, this is less of an issue, but anyone considering Breast Implant Removal should know that it will not usually restore the breasts to their pre-augmentation shape, especially if the Breast Implants have been in for a while. Breast Implant Removal is surgically very easy; however, when sagging is a problem, it may be necessary to add a Breast Lift. For more about Breast Implant Removal, visit San Francisco Breast’s Breast Implant Removal Page. The incisions used for Breast Augmentation are selected because they allow for safe and predictable results, and because they heal well most the time. The incisions used for Breast Lifts and Breast Reductions are much longer, and as a result, are more likely to require Breast Scar Revision. Breast Augmentation Scar Revision Before and After Pictures Left: Irregular light (hypopigmented) scar placed too high makes them obvious. Right: After scar revision the scars are thin and placed at the edge of areolar making them difficult to see. Scar revision of breast scars is no different from scar revision elsewhere on the body. Carefully planning, surgical skill and post-operative care, makes most patients happy with the appearance of their scars. A small percentage of the time, there may a benefit to Breast Scar Revision. For about where breast scars are placed, visit the Breast Augmentation Incisions Page More information about Breast Scar Revision is available on the Breast Scar Revision Page. While Breast Augmentation can rejuvenate deflated breasts, it does not prevent the breast from aging. The natural changes that normally occur in breasts, will continue to occur. Breast Augmentation Revision is more common for Breast Implants with volumes greater than 350 ml. When the implant itself drops due to gravity, “bottoming-out” occurs; however, when the implant remains in the proper position, but the breast itself drops, this is called ptosis (sagging). Just like in women without Breast Implants, ptosis more likely the more natural breast tissue you have. Breast Augmentation with Breast Lift Before and After Pictures Left: The typical postpartum breast is smaller, lower and looks deflated. Right: Breast augmentation alone would leave the nipple low, so a breast lift was used with the breast implants to rejuvenate the breasts. Breast Ptosis, with or without Breast Implants, is treated with a Breast Lift. When Breast Augmentation and a Breast Lift are combined, it is called Breast Augmentation Mastopexy. Sometimes the Breast Lift is combined with Breast Augmentation Revision to get the optimal results. For more about Breast Lifts combined with Breast Implants visit our Breast Augmentation Lift Page.
Breast Implant Replacement – Size and Style Changes
Elective Breast Implant Replacement

Semi-Elective Breast Implant Replacement

Urgent (Non-Elective) Breast Implant Replacement

Breast Implant Revision Surgery for Breast Implant Deflation

Breast Implant Warranty Information
Breast Implant Revision Surgery for Capsular Contracture

Breast Implant Revision Surgery for Breast Implant Malposition

Breast Implant Revision Surgery for Rippling
Breast Implant Revision Surgery for Infection/Exposure
Breast Implant Removal

Breast Scar Revision

Breast Augmentation Revision – Breast Augmentation Lift